We Celebrate Women Entering STEMM. But Do We Help Them Stay?
- Paola Mina-Osorio
- Jun 3
- 6 min read


We celebrate women entering science and medicine. But the harder question is whether our systems allow them to stay, rise, lead, and become mothers without penalty. For Latinas and other underrepresented women, the burden can be even heavier.
Last month, we celebrated Mother’s Day.
We posted photos. Sent flowers. Praised mothers for their strength.
But in STEMM, many systems are still built around constant availability. That design can turn motherhood and caregiving into career penalties.
Not always openly. Not always intentionally. But predictably.
Many women do not leave STEMM because they lack ambition. They leave because the system asks them to perform at a high level while giving them little room to be human.
For Hispanic/Latina women, the pressure can carry added layers. Many women in STEMM face gender bias and caregiving expectations. Latinas may also be navigating cultural expectations, immigration history, financial pressure, underrepresentation, and the burden of being “the only one” in the room, and often “the first one” in the family.
The issue is not who struggles more.
The issue is whether our systems are honest about the different pressures women carry.
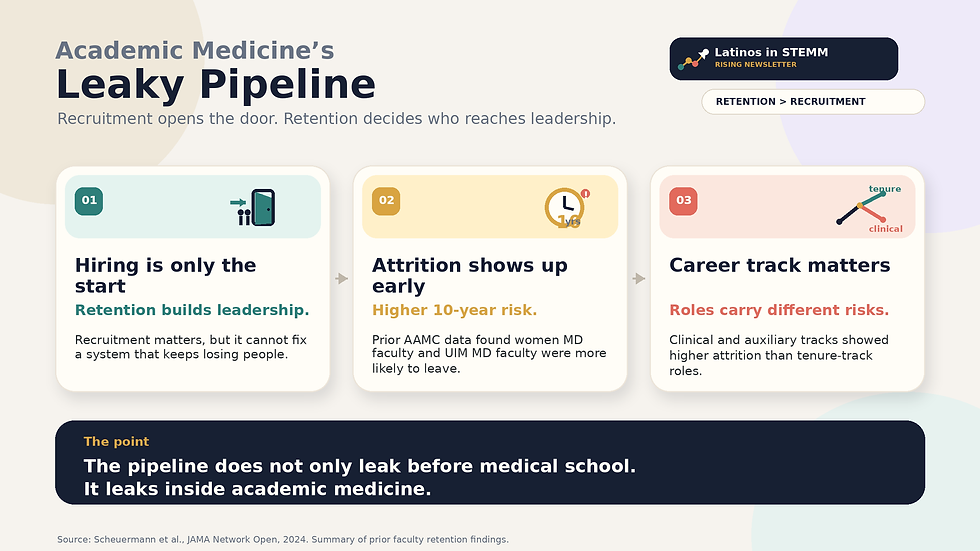
1. Recruitment Opens the Door. Retention Decides Who Advances.
The retention gap is not theoretical.
A 2024 JAMA Network Open study examined 390,766 full-time faculty members at U.S. medical schools from 1978 to 2021. The study found that women left academic medicine about one year earlier than men, and that White faculty had the longest median retention.
Faculty underrepresented in medicine left academic medicine 1 to 4 years earlier than White faculty.
That difference may look small on paper.
But in academic medicine, one year can mean a missed promotion cycle, a lost grant renewal, a leadership opportunity never offered, or a mentor no longer available to the next generation.
The pipeline does not only leak before medical school. It leaks inside academic medicine.
The pattern is not new. Earlier studies had already shown higher attrition among women and underrepresented faculty.
The JAMA study adds another important point: academic medicine is not made up only of physicians. About 25% of medical school faculty are not MDs, so studies focused only on MD or clinical faculty can miss part of the STEMM workforce. Other research has also found that faculty track also matters, with clinical and auxiliary-track faculty at higher risk of attrition than tenure-track faculty.
This pattern does not end after training. As I argued in a previous article on the Latina leadership ceiling, Latinas hold only about 1% of C-suite roles because the pipeline narrows at every stage.
2. Burnout Has Improved, But the Gender Gap Remains
Recent AMA data show physician burnout has declined overall since 2023, but the burden remains high and unevenly distributed.
In 2025, 41.9% of physicians reported at least one symptom of burnout, down from 43.2% in 2024 and 48.2% in 2023. But women physicians were still more likely to report burnout symptoms: 46% of women physicians compared with 37% of men.
That gap matters because many women in STEMM are already resilient. Many Latina women have been resilient their entire lives.
The problem is not that women cannot handle pressure. The problem is that the pressure is not distributed equally.
When women carry more administrative work, more emotional labor, more caregiving responsibility, more bias, and more pressure to prove themselves, burnout is not a personal weakness. It is a predictable outcome.
3. Motherhood Becomes a Career Penalty
Motherhood is often celebrated in public and penalized in private.
The penalty is often hidden because it is framed as a choice.
She chose to reduce hours. She chose not to travel. She chose not to pursue leadership right now.
But choices are shaped by systems.
A woman becomes a mother, or chooses to care for an elderly parent, and suddenly new questions appear: Will she still travel? Will she still publish? Will she still take the stretch role? Will she still be serious about leadership?
This bias may not appear in formal policy, but it shows up in scheduling, promotion decisions, conference travel, after-hours meetings, and who gets offered the next opportunity.
A JAMA Network Open study of early-career physicians found that women were much more likely than men to be working part-time or not employed after training. Among physicians up to six years after completing training, 22.6% of women were not working full-time compared with 3.6% of men. Among physicians with children, the gap widened to 30.6% of women compared with 4.6% of men.

This is not only about personal choice. It is about whether the system makes staying possible.
I know this personally.
I left my corporate career in part because my father and my husband were both facing serious illnesses, and I needed to be present. I was fortunate to have a manager who supported me and encouraged me to take a leave of absence. That support mattered.
But after that time, I realized my family still needed me in a way that would make it difficult to perform at the same level, travel as much, and show up for my team the way they deserved.
4. Prove-It-Again Bias: Who Gets Believed?
There is another layer: the need to prove competence over and over again.
This is often called the "prove-it-again bias." It refers to the pattern in which a person, particularly women and people of color, must repeatedly demonstrate competence to receive the same level of trust or recognition.
A Center for WorkLife Law report on women scientists found that roughly two-thirds of participants reported prove-it-again bias: 66.7% of women interviewed and 63.9% of women surveyed.
For Hispanic women in STEMM, this may look like:
Being mistaken for someone in a lower-status role.
Having expertise questioned in meetings.
Needing more evidence to be trusted.
Being labeled “not ready” despite doing the work.
This matters because systems do not only evaluate performance. They decide whose performance is believed.
Lilly Singh makes a related point in her TED talk, “A seat at the table” isn’t the solution for gender equity. The deeper issue is not only whether women are invited into the room. It is whether the room, the table, and the rules were built for them to succeed.
We cannot invite women into systems that still punish caregiving, difference, and visibility, then act surprised when they leave.
The data are still incomplete. The JAMA Network Open faculty retention study shows gender and racial or ethnic retention gaps in academic medicine, but it does not isolate Latinas compared with White women. That limitation matters because when data fail to name the intersection, the burden becomes easier to ignore.
But the pattern is clear enough: Women leave earlier. Underrepresented faculty leave earlier. Caregiving is not equally supported. Bias affects who is trusted, promoted, and protected.
Together, these forces create a retention risk for many women in STEMM, including Latina women, even when the data fail to name the full picture.
5. What Leaders Are Actually Accountable For
This is not an individual resilience problem.
It is a work-design problem.
The question for leaders is not: How do we help women become more resilient? The better question is: What are we doing that makes talented women leave?
If you lead a team, department, company, lab, or board, retention is visible in your decisions.
Who gets the stretch assignment after becoming a parent?
Who stays in succession planning?
Who gets flexibility without being quietly downgraded?
Who is expected to travel, attend evening meetings, or respond to last-minute requests?
Who receives sponsorship before, during, and after parental leave?
Most organizations respond with programs: another mentoring initiative, another wellness webinar, another statement about supporting women.
Some of these efforts help. But they are not enough if the work design stays the same.
Real change means changing the conditions that push people out:
Normalize flexible work without a career penalty.
Measure who gets high-visibility opportunities, not only who gets hired.
Stop scheduling important meetings at times that punish caregivers.
Make parental leave equal, visible, and usable.
Keep sponsorship active before, during, and after motherhood.
Track who leaves, who stays, who advances, and who disappears from the leadership pipeline.
This is not about lowering standards. It is about removing penalties that were never part of the job description.
The real test is not only whether STEMM can recruit more women. The real test is whether STEMM is mature enough to keep them.
Closing
We cannot celebrate mothers in May and penalize them the rest of the year.
We cannot say we need more women in STEMM while ignoring why so many are pushed out.
And we cannot fix the pipeline if we only focus on entry.
Retention is equity. Advancement is equity. Motherhood support is equity.
Talent is widely distributed. Support is not. Systems decide the difference.
Recommended reading:
Geiger G, Revette A, Nava-Coulter B, et al. Understanding the experience of Latinas in medical education: a qualitative study. https://pubmed.ncbi.nlm.nih.gov/39748490/
Williams JC, Phillips KW, Hall EV. Double Jeopardy? Gender Bias Against Women of Color in Science. Center for WorkLife Law, University of California Hastings College of the Law; 2014. https://worklifelaw.org/publications/Double-Jeopardy-Report_v6_full_web-sm.pdf
Ong M, Wright C, Espinosa LL, Orfield G. Inside the double bind: a synthesis of empirical research on undergraduate and graduate women of color in science, technology, engineering, and mathematics. Harv Educ Rev. 2011;81(2):172-209. doi:10.17763/haer.81.2.t022245n7x4752v2
Geiger G, Sandoval RS, Estrella-Gutierrez N, et al. Latinas in medicine: evaluating and understanding the experience of Latinas in medical education: a cross-sectional survey. https://pmc.ncbi.nlm.nih.gov/articles/PMC10765906/
Gencel-Augusto J, Minaya NJ, Johnson DE, Grandis JR. Underrepresentation of Hispanic women in science, technology, engineering, mathematics, and medicine. https://pubmed.ncbi.nlm.nih.gov/39785094/
Sharp S, Clarke AH, Okoruwa OP. Why do I need to belong? Black women and Latinas navigate medical education beyond belonging toward rightful presence. BMC Med Educ. 2025;25:1205. doi:10.1186/s12909-025-07781-9.
Abraído-Lanza AF, Echeverria SE, Flórez KR, Mendoza-Grey S. Latina women in academia: challenges and opportunities. Front Public Health. 2022;10:876161. doi:10.3389/fpubh.2022.876161.



Comments